Restorative Dentistry
In restorative therapies, we employ the most advanced plastic filler materials, composite resin, glass ionomer cements and amalgam from world-renowned manufacturers.Composite “white” fillings:
- are a highly aesthetic, durable and safe material suitable for the reconstruction of all teeth
- are the material of first choice in restorative therapy not only for front teeth, but also for lateral segments of teeth
- bind to the hard dental tissues /dentin, enamel/ reinforcing the weakened tooth. This allows for removing only the carious bearings of the tooth.
- are highly aesthetic, offering a wide range of colors, which makes it possible to perfectly match your other teeth
- Drawbacks of these materials include the need for precise technique performed whilst restoring the teeth and the requirement to keep the tooth completely dry. Therefore, when treating teeth with white fillings,
 rubber dam is used as standard.
rubber dam is used as standard.
Glass ionomer fillings:
- “White” fillings containing fluoride ions. Thanks to their ability to adhere to hard dental tissues and their anti-decay effects, they are used mainly in the treatment of deciduous teeth in young patients.
- For their relatively low mechanical strength, they are only used as temporary fillings for adult patients.
Amalgam fillings:
- Despite current white filling aesthetics trends and some disadvantages of amalgam fillings, there are still cases where such fillings are used as the safest solution.
- We use quality capsule amalgam with minimal adverse effects.
- We pay attention to the precision of execution consisting both of the tooth shape restoration and the final adjustment of the filling surface.
- Such amalgam fillings are of high quality and last for many years.
Root canal treatment /endodontics/
When is endodontics needed?
- When the caries penetrates to the dental pulp and leads to irreversible damage - dental pulp inflammation /acute pulpitis/ accompanied by intense sustained pain often not retreating until pain killers /analgesics/ are administered.
- When there are no signs of vitality in dental pulp - the tooth is “dead”.
- When there are no signs of vitality in dental pulp and the contents of the pulp cavity and the root canal are heavily contaminated with bacteria diagnosed by the periapical clearing as a “dental follicle”.
- In case of planned prosthetic dental reconstruction /crowns, bridges/ when we are planning the costly reconstuction anchored to often inappropriately tilted teeth with an uncertain biological factor - ie. different prognosis. The purpose of this treatment is to maximize the longevity of the prosthetics.
- If an accident results in the opening of the pulp cavity of the tooth and its subsequent bacterial contamination by oral bacterial microflora.
- When it is necessary to redo the root canal treatment because of an unsatisfactory outcome or the failure of primary treatment. This helps us prevent potential future complications /pain, swelling/.
In all these cases it is necessary to clean up the contents of the pulp cavity, do the root canal system treatment of the tooth and fill the resulting space with hermetic, three-dimensional filling. Currently, there are many methods of root canal treatment (cold and warm gutta-percha) that can painlessly, using new materials and advanced technologies (
 rubber dam,
rubber dam,  apex locator,
apex locator,  endomotor,
endomotor,  magnifying optics,
magnifying optics,  X-ray device with a highly sensitive digital sensor), maintain the affected tooth in function. Subsequent precise reconstruction of the tooth destructed by decay (post-endodontic treatment) is a guarantee of a long-term, functional and successful treatment of the affected tooth.
X-ray device with a highly sensitive digital sensor), maintain the affected tooth in function. Subsequent precise reconstruction of the tooth destructed by decay (post-endodontic treatment) is a guarantee of a long-term, functional and successful treatment of the affected tooth.
3/2011; tooth 36 with “follicle” immediately after the root canal filling
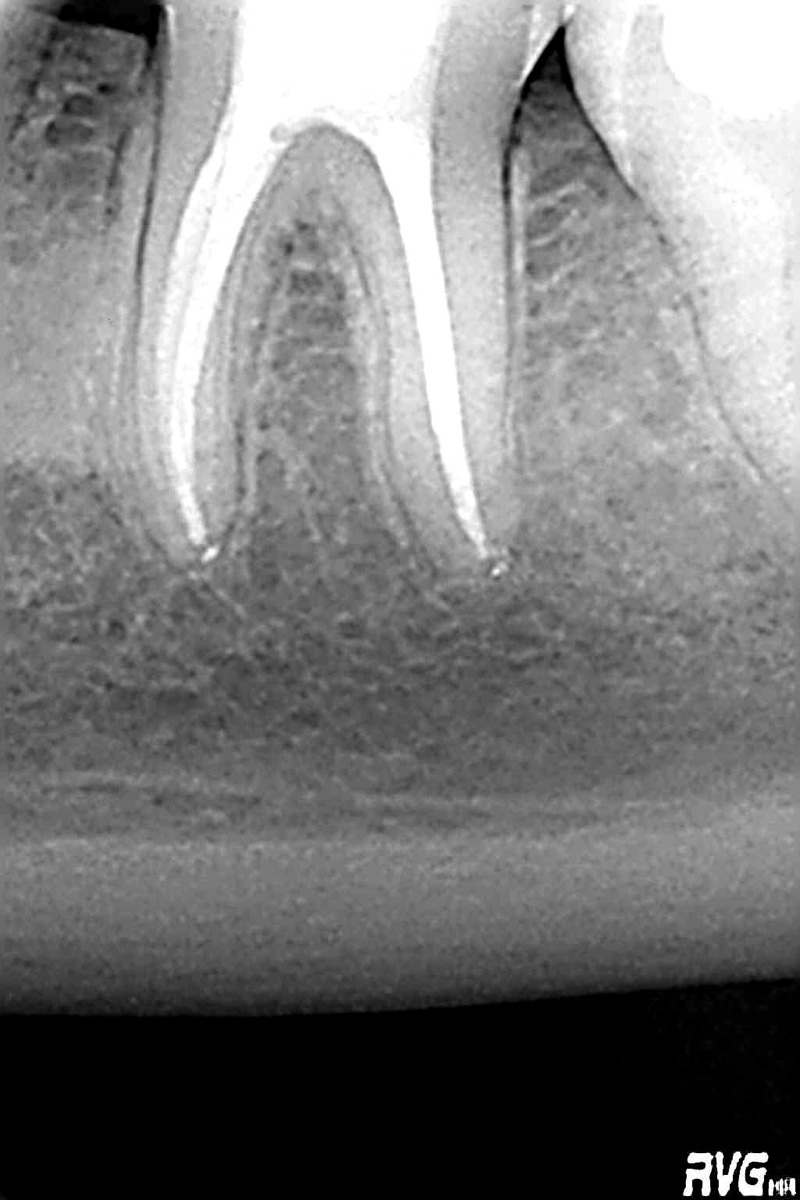
2/2013; working tooth 36 with no complications